symptomatic neuroma procedures
Symptomatic neuromas can cause significant chronic pain and negatively impact patient quality of life. Chronic nerve pain is difficult to manage with traditional pain management options, and historical surgical options may result in neuroma recurrence and don’t allow for recovery of function. Addressing the root cause of nerve pain with contemporary procedures that address the needs of the nerve is an important paradigm shift for treating symptomatic neuromas.
Neuromas can result in debilitating pain and sensory or function loss. When treating neuromas, the surgical treatment option will vary depending on the degree of disorganized neural tissue, anatomic location and whether the nerve can be reconstructed.
Symptomatic neuromas can be treated with neuroma excision and nerve stump reconstruction procedures using Avance® Nerve Graft and Axoguard Nerve Connector® when a distal target is available. Surgically removing the neuroma removes the pain signal and reconstructing the nerve provides the opportunity to recover function.1
remember the following:
- Reconstructing the nerve after excising a neuroma has shown the highest rate of success compared to excision alone or muscle/bone transposition, as determined by postoperative pain, number of revision surgical procedures required and DASH scores.2
- When excising a neuroma, it’s important to reconstruct the nerve to give the patient the opportunity for sensory and motor recovery.
- Reconstruction with Avance Nerve Graft showed 95% meaningful recovery† after neuroma excision.3
solutions
 Avance Nerve Graft®
Avance Nerve Graft®  Axoguard Nerve Connector®
Axoguard Nerve Connector®  Axoguard Nerve Protector®
Axoguard Nerve Protector®  Axoguard HA+ Nerve Protector™ See sizing and IFU on solution pages
Axoguard HA+ Nerve Protector™ See sizing and IFU on solution pages A stump neuroma is an entangled mass of disorganized axons and fibrous tissue that forms at the end of a non-reconstructable peripheral nerve that can cause debilitating pain.4 Despite more than 30 different treatment methods,5 symptomatic neuromas continue to be an unresolved problem in microsurgery that may result in debilitating pain and decreased quality of life.6
When no distal target is available to allow the nerve to be reconstructed after a neuroma is excised, the needs of the proximal nerve end should be addressed to prevent recurrent symptomatic neuroma formation. Surgical options such as traction neurectomy, or cut and bury techniques, do not reduce the development of a new neuroma on the proximal nerve end.7 The Axoguard Nerve Cap® is specifically designed to reduce the likelihood of painful neuroma formation by isolating and protecting the nerve end from surrounding environment.
remember the following:
- 46% of patients who had their hand neuroma simply excised or excised with nerve ends implanted into local muscle tissue saw no improvement in symptoms8 and only 33-40% of patients were satisfied with treatment after burial into muscle or bone.9
- Results from literature indicate residual pain after neurectomy can occur in up to 37% of patients.10
- Neuromas are the number one cause of pain in amputees, also leading to inability to use prosthesis.11,12
The patient had increasing hypersensitivity after traumatic amputation of the left thumb, until a resection of two digital nerve neuromas, one recurrent, with placement of the Axoguard Nerve Cap was successfully performed. Case study courtesy Mark S. Rekant, M.D., Philadelphia Hand to Shoulder Center.
view case study 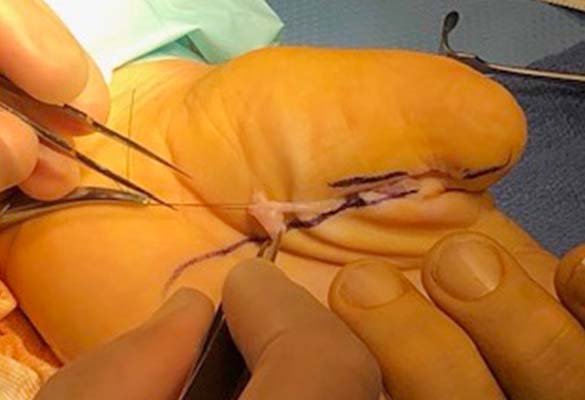
![]()
helping your patients
understand nerve pain
Resources, including patient testimonials and FAQs, can be found at rethink-pain.com. Printed brochures are also available to provide to your patients. Contact your sales rep or visit the Rethink Pain site to download copies.
learn more 
more procedures
There’s only a short form between you and our nerve product team who can help you get more information about our nerve repair solutions.
references
†Defined as Medical Research Council Scale of S3/M3 or greater.
- Challoner T, et al. The surgical management of traumatic neuromas. J Musculoskelet Surg Res. Feb 2019;3:22-29.
- Guse DM, et al. Outcomes of the surgical treatment of peripheral neuromas of the hand and forearm: a 25-year comparative outcome study. Ann of Plast Surg. 2013;71(6):654-658.
- Safa B, et al. Peripheral nerve repair throughout the body with processed nerve allografts: Results from a large multicenter study. Microsurgery. Jul 2020;40(5):527-537.
- Ducic I, et al. The role of peripheral nerve surgery in the treatment of chronic pain associated with amputation stumps. Plast Reconstr Surg. Mar 2008;121(3):908-914.
- Starr BW, et al. Traditional Neuroma Management. Hand Clin. 2021;37(3):335-344.
- Wojtkiewicz DM, et al. Social impact of peripheral nerve injuries. Hand (N Y). 2015;10(2):161-167.
- Dellon AL, et al. Treatment of the painful neuroma by neuroma resection and muscle implantation. Plast Reconstr Surg. 1986;77(3):427-438.
- Laborde K, et al. Results of surgical treatment of painful neuromas of the hand. J Hand Surg Am. Mar 1982;7(2):190-193.
- Stokvis A, et al. Surgical management of neuroma pain: a prospective follow-up study. Pain. Dec 2010;151(3):862-869.
- Bucknall V, et al. Outcomes following excision of Morton’s interdigital neuroma: a prospective study. Bone Joint J. Oct 2016;98-B(10):1376-1381.
- O’Reilly MA, et al. High-resolution ultrasound findings in the symptomatic residual limbs of amputees. Mil Med. Dec 2013;178(12):1291-1297.
- Geraghty TJ, et al. Painful neuromata following upper limb amputation. Prosthet Orthot Int. Dec 1996;20(3):176-181.